
by: Peter Lembke, VitalremedyMD Inc, Boca Raton, FL (copyright)
February 10th, 2021
Summary
An ideal omega-3 supplement should contain highly concentrated EPA and/or DHA, preferably in the re-esterified rTG-form. The original source of the omega-3 fatty acids in the final concentrated rTG supplement is not of major importance. The manufacturer´s recommended daily serving should provide at least 500-1000 mg EPA and/or DHA and such supplement should generally be taken during or shortly after a main meal.
Very efficient and highly concentrated EPA+DHA pharmaceutical drugs in the ethyl-ester or EE-form, should always be taken together with a main meal in order to maximize bio-absorption of the essential fatty acids.
Introduction:
Half a century has passed since Dyerberg and Bang [1] suggested for the first time a possible correlation between the low incidence of coronary heart disease among Greenland Inuit population and their elevated intake of omega-3 fatty acids from marine sources. The researchers found a major difference in the fatty acid composition in the blood of native Greenlandic West-Coast Inuit´s compared to Inuit´s living in Denmark. The main difference observed was the very high concentration of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) in the serum of the native population living in Greenland. Soon thereafter it was observed that this high EPA and DHA content measured in their blood went back to their traditional diet, rich in marine fats (fatty fish, seals, whale, etc.).
The only significant natural sources for these two essential Omega-3 fatty acids, were at that time and still are today, found in cold water marine animals like sardine, anchovy, salmon, herring, tuna, squid, certain algae and krill. Unfortunately fatty fish and other marine foods are no more very popular in modern western diets [2]. The consequence is a general deficiency in omega-3 fatty acids found in the western population. A good and safe way to overcome this deficiency is to take on a regular basis a high quality nutritional supplement, rich in omega-3. However, consumers and health professionals get confused by the large variation of different omega-3 /fish oil products offered in the market. The choice of products seems endless:
Omega-3 products found on the market come from:
- Fish oil
- Tuna,
- salmon,
- sardines,
- anchovy´s,
- herring´s
- cod liver oil
- Squid oil
- Krill oil
- Algae oil
- Seal Oil
From the biochemical view, it is not of importance from which species originally the EPA/DHA came from in a concentrated omega-3 product. The chemical molecule EPA/DHA is the same no matter if it originated from an algae-, squid-, krill- or a herring oil. From the potential contamination threat (heavy metals, dioxins, PCB´s, etc) however it is always better to choose small fish species that have a shorter life-cycle. Large fish like tuna and salmon live many years in the ocean and have plenty of time to accumulate these contaminants in their body fat. Also, from a sustainability standpoint it is better to choose smaller, rapid replicating, species like sardines, anchovies, herring, squid and algae because the risk of over-harvesting these small species is far lower than in case of the larger fish.
All of the above listed marine oils are available in different chemical forms such as:
- ethyl ester (EE),
- natural triglyceride (TG),
- re-esterified TG (rTG),
- free fatty acid (FFA),
- phospholipids (PS),
- mono-glycerides (MG), …
Additionally, one has to distinguish between different delivery forms:
- Softgels (bovine-, fish-, porcine-, vegetable-gelatin)
- Liquid oils
- Emulsions
- Powders
What makes it even worse is that the oil or omega-3 concentrates coming from different species have different fatty acid compositions (EPA & DHA content). Consumer products usually differ in their capsule size and thus oil content. So even if the same oil is used, two products from two different producers may have different absolute quantities of EPA and DHA in one capsule. Finally, each Manufacturer suggests his own daily recommended serving – many times not driven by nutritional needs but more by economic and marketing reasons.
There are endless different brands and prices all claiming to have the best product. The idea of this paper is to provide a little more clarity in the field of choosing the preferable chemical form of the omega-3 fatty acids for their best bioavailability and to discuss the importance of the daily recommended dose given by the manufacturers for these important nutritional supplements.
Production basics of fish oil-/omega-3 concentrates:
In order to understand the reasoning for why there are so many different chemical forms of fish oil- and omega-3 supplements on the market we need to discuss briefly the production process:
Natural fish oils, for example from anchovies, usually contain more or less 18% EPA and 12% DHA. So a total of 30% long chain omega-3 fatty acids. The rest of the oil consists of a mix of other triglycerides composed of saturated-, monounsaturated-, other polyunsaturated fatty acids and cholesterol. In these natural marine oils the EPA and the DHA are usually mainly present in the natural Triglyceride (TG) form. This means you have in average one molecule EPA or DHA bound to one of the three arms of one glycerol molecule. It is practically impossible to substantially concentrate the EPA and DHA content as long as the fatty acids are still bound to the glycerol. Therefore, in order to achieve concentrations above roughly 30-35% of EPA+DHA there is no other way than to split the natural TG into fatty acid ethyl ester (EE) and glycerol, in the presence of ethanol and a catalysator or enzyme (lipase). The created mix of fatty acid ethyl ester (FAEE) are now “free” and no longer bound to the glycerol. As they differ in molecular weight, chain-length and degree of saturation it is now possible to separate the mixture and achieve purities of each fatty acid ethyl ester going up to almost 99% [3]. Table 1 Shows some of the most common separation technologies and the achievable concentrations of EPA and DHA reflected in the final consumer product.
|
Technology |
EPA content |
DHA content |
EPA+DHA |
|
Short-path- or Molecular Distillation |
33% |
22% |
50-55% |
|
|
55% |
10% |
60 – 70% |
|
|
70% |
<5% |
70% |
|
Supercritical Fluid Chromatography (SFC) |
Up to 99% |
Up to 95% |
Up to 99% |
|
Column Distillation |
Up to 99% |
Up to 95% |
Up to 99% |
|
Winterization |
33% |
22% |
50-55% |
Table 1: most popular separation techniques and achievable EPA and DHA concentrations in %.
No matter which technology was applied, all resulting EPA and/or DHA concentrates shown in Table 1 are in the EE-form (see Figure 1 ). Many omega-3 supplement or pharma product producers use this chemical form of the concentrated EPA and DHA in their final formulation. This is the most practical and cheapest way for them. Converting the EE back into Omega-3 rTG concentrates means additional manufacturing steps, product yield loss and at least a 20% increase in their production costs.
In order to differentiate between the original natural TG-form and the re-esterified rTG-form they are usually called “re-esterified TG´s”, “re-constituted TG´s” or simply “rTG”. This re-esterification process is basically done in three steps: first the EE are converted to monoglycerides (MG), then to di-glycerides (DG) and finally to the triglycerides (rTG). So depending at what stage you interrupt the transformation process you get a product richer in MG´s, DG´s or rTG´s. All these different chemical forms of omega-3 fatty acids are found and commercialized on the market.
On the other hand, you can also easily convert the EPA-/DHA-EE concentrates chemically or with the help of enzymes into the FFA form which is found mainly in some pharma formulations.

Literature Review and determination of a “Relative Bioavailability Index”
In order to compare the results of the literature research carried out, we determined a “Relative Bioavailability Index”. In most papers the absorption behavior between concentrated ethyl-ester (EE) and other chemical forms like TG´s or FFA´s were studied. The reason why most studies included the omega-3 EE is that almost all pharmaceutical approved omega-3 drugs are in the EE-form.
We gave the EE a Relative Index of 100. If for example the bioavailability of a rTG-product was twice as good as the compared EE-product, then the TG-product became a Relative Bioavailability Index of 200. If on the other hand the bioavailability of the FFA-form was only 80% of the compared EE, the FFA became an Index of 80. In this way it was possible to compare the different results obtained in these studies and see certain tendencies regarding the relative bioavailability of the various chemical forms of the EPA/DHA. It is important to note, that the ”Relative Bioavailability Index” only provides an idea of which chemical form was better absorbed in comparison to the other investigated forms, under the defined conditions. It does not provide any information on the absolute amount in “mg” of EPA/DHA absorbed.
Observations:
Table 2 is separated in two parts. The upper part reflect the outcomes from studies carried out in the fasted state. The lower part of the table shows the observations made with subject in the fed state. This is important because the bioavailability of omega-3 fatty acid supplements and pharma drugs in the EE-form varies strongly in the fed and fasted state. In the fasted state the bioavailability of the TG-form (mainly standard 18/12-fish oil supplements ) is up to 3,5-times better compared to the EE-form [9, 10]. It is interesting to note that in the few studies that analyzed the difference in bioavailability between the natural triglycerides (TG) and the reconstituted triglyceride form (rTG) (mostly found in premium concentrated omega-3 supplements) indicate that there is a slightly preferred bioavailability seen with the rTG-form [1, 12, 13]. Further studies need to confirm this observation. Even more dramatic is the difference in bioavailability in the fasted state between EE and FFA (Figure 2). On empty stomach the free fatty acids (FFA) are in average 5-times more bioavailable than the EE-form [7, 8, 9, 10]. Unfortunately do the omega-3 oils in the FFA-form have a very intensive, aggressive fishy taste and provoke fishy burps which makes this chemical form for most nutritional supplements not of interest. However, with an appropriate enteric coating of the gelatin shell of the soft gel capsule new pharmaceutical formulations have been successfully developed.
In the lower half of Table 2 we have listed the Relative Bioavailability Index ability for studies carried out in the fed state. In the fed state, the difference between the bioavailability observed between the EE and FFA is not so pronounced as previously discussed in the fasted state. However the TG-form is still approximately 2-3 times more absorbed compared to the EE [9,10].
|
Authors |
Year |
Subjects |
Diet |
rel. EE-INDEX |
rel. FFA INDEX |
rel. TG INDEX |
rel. rTG INDEX |
|
J Dyerberg et al |
2010 |
72 |
100 |
125 |
137 |
170 |
|
|
J Neubronner et al |
2011 |
150 |
100 |
106 |
|||
|
J.F. Lapointe et al |
2019 |
56 |
fasted state |
100 (EPA) |
681(1) |
||
|
J.F. Lapointe et al |
2019 |
56 |
fasted state |
100 (DHA) |
243(1) |
||
|
J.F. Lapointe et al |
2019 |
56 |
fasted state |
100 (EPA+DHA) |
480(1) |
||
|
M.H. Davidson et al |
2012 |
54 |
low fat diet |
100 |
400 |
||
|
E. Offman et al |
2013 |
52 |
low fat diet |
100 |
580 |
||
|
L.D. Lawson et al |
1988 |
8 |
low fat |
100 (EPA) |
475 |
340 |
|
|
L.D. Lawson et al |
1988 |
8 |
low fat |
100 (DHA) |
475 |
285 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
J.F. Lapointe et al |
2019 |
56 |
fed state |
100 (EPA) |
100(1) |
||
|
J.F. Lapointe et al |
2019 |
56 |
fed state |
100 (DHA) |
100(1) |
||
|
J.F. Lapointe et al |
2019 |
56 |
fed state |
100 (EPA+DHA) |
85(1) |
||
|
M.H. Davidson et al |
2012 |
54 |
high fat diet |
100 |
130 |
||
|
L.D. Lawson et al |
1988 |
8 |
high fat |
100 (EPA) |
158 |
445 |
|
|
L.D. Lawson et al |
1988 |
8 |
high fat |
100 (DHA) |
158 |
285 |
|
|
J. Neubronner |
2010 |
150 |
fed state |
100 |
115 |
||
|
W.S. Harris |
2007 |
23 |
fed state |
100 |
103 |
||
|
L.M.Arterburn |
2008 |
32 |
fed state |
100 |
100 |
||
|
J. Dyerberg et al |
2015 |
120 |
fed state |
100 |
110 |
||
|
|
|
|
|
|
|
|
Table 2 reflects the findings of numerous studies on the bioavailability of the two omega-3 fatty acids EPA and DHA in the years between 1988 and 2019.
We only found two studies [12, 13] comparing directly the difference in bioavailability of TG and rTG in the fed state. In both cases there was no difference observed in their absorption behavior. Together with the results reported with fastened subjects in Table 2, where rTG actually showed a better absorption behavior compared to the natural TG-form [1, 2], this indicates that the rTG is at least as bioavailable as the natural TG in the fasted and fed state.

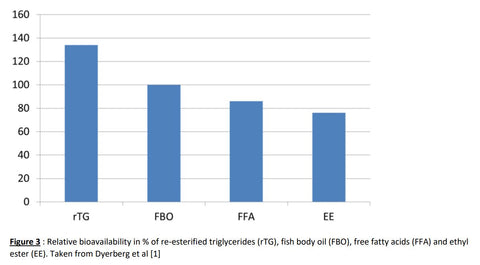
Dyerberg et al published in 2010 probably one of the most cited studies [1] regarding the different bioavailability’s found in natural fish body oil (FBO), rTG, EE and FFA. In this double-blind study 72 subjects received on a daily basis, during two weeks, a defined quantity of EPA+DHA (3,3 g/day), however in different chemical forms. Figure 3 indicates that the rTG-form of the EPA supplement was best absorbed and better incorporated into the sum of serum lipids. Followed by the natural triglyceride fish body oil (FBO) and FFA. The EE form showed the poorest bioavailability among the studied supplements

Fasted State versus Fed State
An important finding in the majority of studies trying to understand the absorption behavior of omega-3 ethyl ester (EE) was that it is of utmost importance to take the omega-3-EE medication after a fatty meal (fed state) and not on empty stomach (fasted state). Unfortunately this fact is not detectable from the data shown in Table 2 because the Relative Bioavailability Index for the EE-form was always set to 100, even if the bioavailability with respect to absorbed absolute quantity of omega-3 (in mg) was very poor. A good illustration of this food effect can be seen in the absorption charts from the ECLIPSE study [18] where the bioavailability between an omega-3-ethyl ester drug (EE) and a omega-3-free-fatty-acid drug (FFA) was compared. The total EPA and DHA content of both drugs are comparable. From Figure 5a can be seen that the EE formulation (green line) in the fasted state (low fat diet) is only very poorly absorbed. Whereas the FFA form gets well absorbed with a typical Cmax at approx. 5 hours after intake. Taking the same formulations after a high fat diet (fed state) the absorption behavior of the EE improves dramatically and shows a similar curve-shape than the FFA-form (Figure 5b). However, looking at the total EPA+DHA plasma concentrations of the two charts (Y-Axis), it also becomes clear that the absolute quantity of absorbed EPA-FFA and DHA-FAA (in mmol/ml blood) improves almost twofold when the drug is taken after a fatty meal.

Therefore, in order to maximize the absolute quantity of EPA+DHA absorbed into the blood one should always ingest the omega-3 nutritional supplement or pharmaceutical drugs together or shortly after a fatty meal. Our digestive system, in particular the pancreatic enzymes and bile acids need to be triggered and released by a minimum amount of fat in our diet. This is especially important for the omega-3 EE form. Taking such a supplement or drug before or after a light breakfast (for example only fruit and coffee) will not release any pancreatic lipase that can split the EE into the absorbable FFA form. The majority of the ingested omega-3-EE will thus not be able to be absorbed and are lost with the feces. On the other hand, products offered as TG or rTG start to provoke a pancreatic response even in a fasted state and thus can be absorbed after being converted to the FFA and monoglyceride form. The efficiency of this “lipid digestion” can be even more improved by taking the TG/rTG omega-3 together with a fatty meal. In this case a maximum pancreatic lipase activity can be achieved which maximizes the efficiency of transforming EPA/DHA-rTG into the bioabsorbable FFA and MG esters. However, many people taking omega-3 products suffer from hyperlipidemia and thus should avoid a too fatty diet. In this case the omega-3 supplement/drug should be ideally in the FFA-, TG- or rTG-form.
As general rule can be said, that all EPA and/or DHA chemical forms are far better absorbed and thus more bioavailable, if taken together with or shortly after a fatty meal (Figure 6). Thus, bioavailability is directly influenced by (i) the chemical form of the omega-3 fatty acid and (ii) whether this omega-3 fatty acid was ingested in the fasted or fed state.

Concentrated rTG products are not “… just another fish oil…”. The absolute amount of ingested EPA+DHA matters.
A randomized clinical trial to determine the efficacy of manufacturers’ recommended doses of omega-3 fatty acids from different sources was published by Laidlaw et al in 2014.[15]
This different, but also very important approach, studied the percentage change of EPA and DHA from baseline values in whole blood plasma after consuming four different Omega-3 supplements according to their recommended or prescribed daily dose.
- Concentrated Triglyceride (rTG) fish oil: (R.D.I.) EPA of 650 mg, DHA of 450 mg
- Ethyl Ester (EE) fish oil: (R.D.I.) EPA of 756 mg, DHA of 228 mg
- Phospholipid (PL) krill oil: (R.D.I.) EPA of 150 mg, DHA of 90 mg
- Triglyceride (TG) salmon oil: (R.D.I.) EPA of 180 mg, DHA of 220 mg
(R.D.I.) = Recommended Daily Intake by the producer of the supplement
Figure 7 shows clearly that the concentrated rTG supplement produced a greater increase in whole blood omega-3 fatty acids than the rest of the compared products. Focusing on the EPA alone, Figure 7 shows that both rTG and EE supplement result in a strong increase of EPA in the serum lipids. This was to be expected because both the rTG and the EE product contain the highest quantity of EPA. Additionally, the trial was carried out in the fed state so a part of the lower bioavailability of the EE was compensated by the fat content in the subjects diet. Nevertheless, in spite of the fact that the EE-product contained 106 mg more EPA per recommended dose than the rTG-product, the latter demonstrated the highest EPA incorporation into the whole blood serum. The standard fish oil capsules and krill oil capsules ingested at their recommended dose showed dramatically lower results.
When analyzing the change of DHA concentration in the serum, again the rTG supplement shows an almost 4-fold better incorporation than the EE or the standard fish oil capsule. Krill oil showed the lowest increase of DHA in the serum. This finding was to be expected because the concentration of EPA and DHA in the different formulations varied dramatically. Especially Krill Oil, characterized by a high phospholipid content and thus good absorption properties, shows unfortunately a very low EPA+DHA content. So the good bioavailability of Krill Oil cannot compensate a lack of EPA+DHA in the formulation. In this case the Krill Oil supplement producer should recommend a much higher daily dose (more capsules/day). This however would increase significantly the costs for the consumer and/or decrease the margins for the producer. Both would make the product less attractive for the consumer and producer. From the pure health perspective, an increased daily dose recommendation for this product would be the best solution.
For preventive applications many health professionals recommend a daily serving of 500-1000 mg EPA and/or DHA. For therapeutic applications the daily recommended serving often exceeds 3000-4000 mg EPA and/or DHA per day.

Although the above discussed finding from the Laidlaw study seem obvious, in reality many consumers and even health professionals still consider all omega-3 products as if they are “…simply/mostly the same…” and are all “…just fish oils…”. Laidlaw et al showed clearly that this is not the case. Absolute Quantity in mg per serving matters!
In order to increase the probability that recommended daily servings of 500 to 4000+ mg EPA and/or DHA really end up in our blood stream and are thus bioavailable for our body organs, it is very important that the omega-3 supplement we chose has a
- high concentration of EPA and DHA (in mg per gram),
- a sufficiently large capsules size,
- is taken together with a main meal and
- the concentrated omega-3 fatty acids should be preferably in the rTG-form.
Conclusion
In order to evaluate the bioavailability of an omega-3 supplement, which is generally measured as the amount of omega-3 fatty acids EPA + DHA (in mg) being incorporated into the whole blood serum after ingesting a recommended daily dose or serving, one has to consider:
- Absolute amount of EPA and DHA (in mg) per daily serving. This depends on the volume and the milligram of EPA and DHA in the oil found inside the supplement soft gel capsule. Additionally, keep in mind a daily serving can be 1, 2 and more capsules.
- Bioavailability of chemical form of the omega-3´s (EE, TG, rTG, FFA,…).
- Administered in the fed- or fasted state.
After analyzing some of the most important scientific papers published in this field over the last 30 years, we suggest the following order of bioavailability for omega-3 nutritional supplements:
In the fed state : rTG > TG >FFA > EE
In the fasted state : FFA >rTG > TG > EE
Generally all omega-3 supplements, regardless of their chemical form, are better bioavailable in the fed state than in the fasted state. For further information regarding the bioavailability of omega-3 fatty acids the interested reader is referred to reviews such as from Punia et al [19] and Schuchardt et al [20].
Literature:
[1] J. Dyerberg, H.O. Bang. Plasma Lipid and lipoprotein pattern in Greenlandic West-Coast Eskimos, The Lancet, vol. 297, issue7710: 1143-1146]
[2] M Thompson et al. Omega-3 Fatty Acid Intake by Age, Gender, and Pregnancy Status in the United States: National Health and Nutrition Examination Survey 2003–2014. Nutrition (2019) 11(1): 177
[3] P Lembke. “Production Techniques for Omega-3 Concentrates” in Omega 6/3 Fatty Acids: Functions, Sustainability Strategies and Perspectives. F De Meester et al (eds.) DOI 10.1007/ 978-1-62703-215-5_19, Springer Science + Business Media New York (2013): 353-364
[4] E. Offman et al. Steady-State bioavailability of prescription omega-3 on a low fat diet is significantly improved with a free fatty acid formulation compared with an ethyl ester formulation: The ECLIPSE II Study. Vascular Health and Risk Management, vol 9 (2013): 563-573
[5] J Neubronner et al. Enhanced increase of omega-3 index in response to long-term n-3 fatty acid supplementation from triacylglycerides versus ethyl esters. European Journal of Clinical Nutrition (2011) vol. 65, no. 2: : 247-254
[6] J.F. Lapointe et al. Clinical Therapeutics (2019) vol. 41, no. 3: 426-444
[7] M.H. Davidson et al. Journal of Clinical Lipidology (2012) vol.6, issue 6: 573.584
[8] E. Offman et al. Vascular Health & Risk Management (2013) vol.9: 563-573
[9] L.D. Lawson et al. Human absorption of fish oil fatty acids as triglycerides, free acids, or ethyl esters. Biochemical & Biophysical Research Communications (1988) vol. 152, issue 1: 328-335
[10] L Lawson and B Hughes. Absorption of eicosapentaenoic acid and docosahexaenoic acid from fish oil triglycerols or fish oil ethyl esters co-ingested with a high-fat meal, Biochemical and Biophysical Research Communications, vol. 156, no. 2 (Oct 31, 1988): 960-963.
[11] Wakil A, Mir M, Mellor DD, Mellor SF, Atkin SL: The bioavailability of eicosapentaenoic acid from reconstituted triglyceride fish oil is higher than that obtained from the triglyceride and monoglyceride forms. Asia Pac J Clin Nutr 2010, 19(4):499–505. 26.
[12] W.S. Harris et al. Consumption of salmon v salmon oil capsules: effects on n-3 PUFA and selenium status. Am J Clin Nutr (2007) vol. 86: 1621-1625
[13] L.M. Arterburn et al. Algal-oil capsules and cooked salmon: nutritionally equivalent sources of docosahexaenoic acid. J Am Diet Assoc (2008) vol. 108, issue 7: 1204-1209
[14] A. Hedengran, J. Dyerberg et al. n-3 PUFA Esterified to Glycerol or as Ethyl Esters Reduce Non-Fasting Plasma Triacylglycerol in Subjects with Hypertriglyceridemia: A Randomized Trial. Lipids (2015) vol. 50, issue 2: 165-175
[15] Laidlaw et al. A randomized clinical trial to determine the efficacy of manufacturers’ recommended doses of omega-3 fatty acids from different sources in facilitating cardiovascular disease risk reduction. Lipids in Health and Disease (2014)
[16] Sneh Punia et al. Omega-3 Metabolism, absorption, bioavailability and health benefits - A review. Pharma Nutrition, vol. 10 (Dec 2019)
[17] J.P. Schuchardt et al. Bioavailability of Long_chain fatty acids. Prostaglandins, Leukotrienes, and Essential Fatty Acids, vol 89, issue 1 (2013)
[18] M.H. Davidson. A novel omega-3 free fatty acid formulation has dramatically improved bioavailability during a low-fat diet compared with omega-3-acid ethyl esters: The ECLIPSE (Epanova® compared to Lovaza® in a pharmacokinetic single-dose evaluation) study.. J Clin Lipidol (2012) 6: 573-584
[19] Sneh Punia et al. Omega-3 Metabolism, absorption, bioavailability and health benefits - A review. Pharma Nutrition, vol. 10 (Dec 2019)
[20] J.P. Schuchardt et al. Bioavailability of Long_chain fatty acids. Prostaglandins, Leukotrienes, and Essential Fatty Acids, vol 89, issue 1 (2013)